|

Click weeks 0 - 40 and follow fetal growth
|
||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||
|
April 25, 2013--------News Archive
|
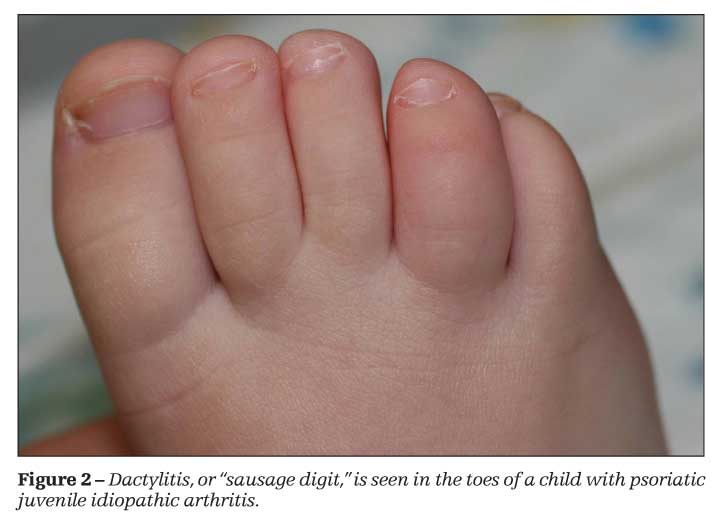
New genetic links to juvenile arthritis Researchers have increased the number of confirmed genes linked to juvenile idiopathic arthritis (JIA) from three to 17 – a finding that will clarify how JIA fits into the spectrum of autoimmune disorders and help identify potential treatment targets. Published April 21in Nature Genetics, the study involves an international research team that analyzed 2,816 JIA cases recruited from more than 40 pediatric rheumatology clinics. It was the largest collaborative patient population of JIA to date, including patient DNA samples from across the United States, Germany and United Kingdom. Susan Thompson, PhD, and researcher in the Division of Rheumatology at Cincinnati Children's Hospital Medical Center leads the study. "These findings will help us understand how the long suspected genetic contributions to JIA are driving the disease process, with the ultimate goal being earlier and improved diagnosis and treatment," Thompson said. JIA is the most common rheumatic disease of childhood that involves several different but related forms. Affecting some 50,000 children in the US, the actual cause of the disease remains unknown. JIA is considered an autoimmune disorder, in which the body's immune system mounts an attack against its own healthy tissues. JIA can be treated with medications and physical therapy, but the disease can persist for many patients into adulthood. Prior to the current study, only three genes were associated with known JIA risk though scientists suspected the likelihood of more gene involvement. The research team used what is known as the Immunochip array to measure variation in the genes (DNA) coding for components of the immune system for 2,816 JIA patients in the study. Those findings were compared to the DNA of 13,000 healthy controls to look for genetic differences. The analyses re-confirmed JIA's connection to the original three genes, identified a link to the 14 new genes and pointed to the possibility that another 11 genetic regions may be implicated. The scientists stressed that their work continues in order to identify additional genetic links, and recently began conducting functional studies to pinpoint disease processes. Although the current study substantially increases the number of confirmed susceptibility genes for JIA, researcher data indicates that additional genetic risk factors still remain to be discovered. Other researchers helping lead the study included Carl Langefeld, PhD, and Miranda Marion, MA, at the Wake Forest School of Medicine, Drs. Wendy Thomson, Anne Hinks and Joanna Cobb at the University of Manchester in the UK, and Sampath Prahalad, MD, at the Emory University School of Medicine. Funding support for the research came, in part, from the U.S. National Institutes of Health (RC1-AR-058587, U01-AI-067 150S1, N01-AR-42272, P01-AR-048929, P30-AR-473639, K23-AR-50177, R01-AR-060893, R01-AR-057106, N01-AR-62277, P30-GM-103510, U19-AI-082714, P30-AR-053483, RP-PG-0310-1002, RC2AR059092, DK062431, DK62422, DK062432, DK06423, DK062429) from the Arthritis Foundation, The Val A. Browning Charitable Trust and the Marcus Foundation. About Cincinnati Children's Original article: http://www.eurekalert.org/pub_releases/2013-04/cchm-isf042413.php |
||||||||||||||||||||||||||||